What Causes Subcutaneous Fat in Women?

Key Takeaways
- Subcutaneous fat makes up 85–90% of total body fat and is the last to go
- For women, hormonal shifts (especially dropping estrogen during perimenopause) actively redirect fat storage toward the belly
- Subcutaneous fat cells in the abdomen have fewer fat-releasing receptors and more fat-retaining receptors than fat elsewhere in the body
You can grab your belly fat. You can pinch it, jiggle it, and feel every last stubborn inch of it — and somehow, it refuses to leave. If that sounds painfully familiar, you’re not alone.
There’s a Reddit thread that went quietly viral, where someone simply wrote: “A reminder that subcutaneous fat is a bitch and is the last to go away. Don’t give up!” — and hundreds of women flooded the comments with relief. Finally, someone said it.
What does Subcutaneous fat look like?
Location: Subcutaneous fat, a type of belly fat is the layer of fat stored directly beneath the skin, above the muscle. It’s the kind you can pinch between your fingers — soft, jiggly, and maddeningly persistent.
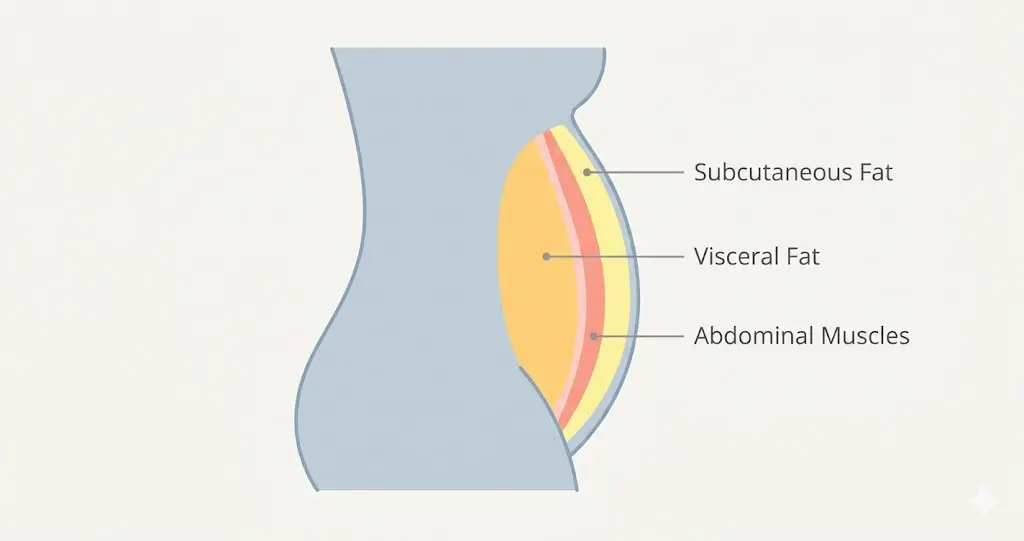
It accounts for roughly 85–90% of your total body fat, according to research published via InBody.
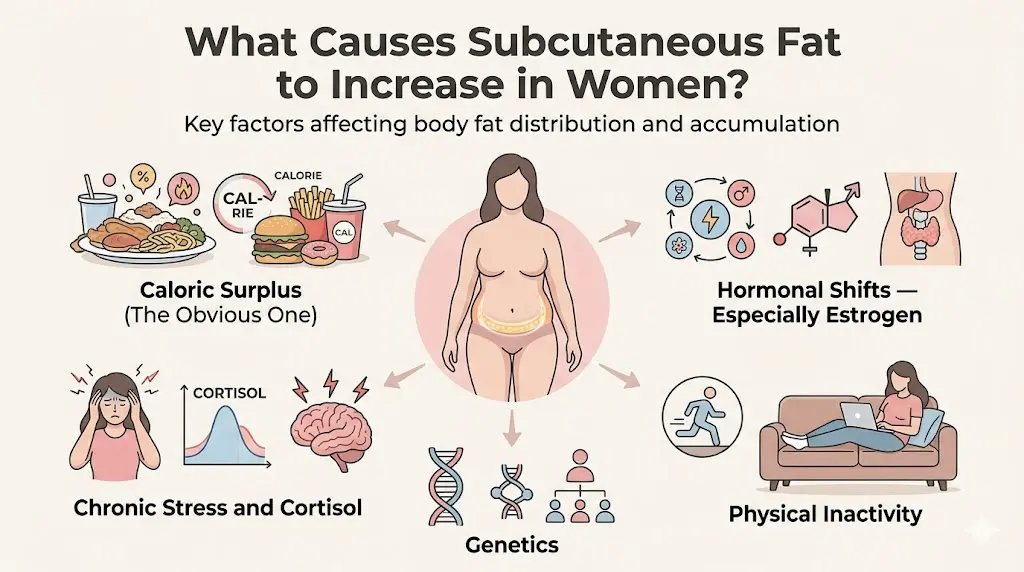
What Causes Subcutaneous Fat to Increase in Women?
Caloric Surplus (The Obvious One)
Consuming more calories than your body burns — consistently — gets stored as fat. Simple carbohydrates, ultra-processed foods, and high-sugar diets accelerate this. The Cleveland Clinic identifies excess calorie intake as the primary driver of subcutaneous fat accumulation. If you are feeling a lil bit hungry before going to bed, you are in calorie deficit.
Hormonal Shifts — Especially Estrogen
This is where it gets uniquely female. Estrogen actively directs fat storage away from the abdomen during a woman’s reproductive years, preferring the hips and thighs. When estrogen drops during perimenopause and menopause, fat storage shifts — often dramatically — toward the lower belly.
Research published in Climacteric confirms that postmenopausal women experience significant redistribution of body fat toward central (abdominal) subcutaneous deposits.
Chronic Stress and Cortisol
Cortisol — your primary stress hormone — doesn’t just affect your mood. Chronically elevated cortisol has been shown to promote the deposition of fat specifically in the abdominal region. A 2000 study in Psychosomatic Medicine found that women with greater abdominal fat had higher cortisol reactivity to stress compared to women with peripheral fat distribution. This matters: if you’re sleeping 5 hours a night and running on anxiety, your fat loss will stall regardless of diet.
Physical Inactivity
Skeletal muscle is metabolically active tissue — it burns calories even at rest. When muscle mass declines (a process called sarcopenia, which accelerates after 30), your resting metabolic rate drops. Less muscle = fewer calories burned = more fat retained. The Mayo Clinic confirms that muscle mass is one of the largest determinants of basal metabolic rate. You are laying on couch for straight 6-10 hours and complaining about belly fat needs to be studied!
Genetics
Fat distribution patterns are substantially heritable. Twin studies have shown that where your body prefers to store fat — and how readily it releases it — is partially written in your DNA. This doesn’t mean you’re stuck. It means your baseline is different from someone else’s, and comparing results is counterproductive.
Reminder: Don’t complain about your forefathers for being bulky, fix your routine buddy.
Why Is Subcutaneous Fat So Hard to Lose?
Subcutaneous abdominal fat cells have fewer beta-adrenergic receptors — the receptors that receive fat-releasing signals from hormones like adrenaline and noradrenaline. Fewer receptors means the cells respond more slowly to fat-burning signals compared to fat elsewhere in the body. As explained by Marco Ellis, MD, this is why you might lose fat visibly in your face or arms before your belly budges. It’s not that you’re doing anything wrong — the belly region is physiologically last in line.
Women also tend to have a higher proportion of alpha-2 adrenergic receptors in lower-body and abdominal subcutaneous fat, which actually inhibit lipolysis (fat breakdown). It’s a feature, not a bug — evolutionarily designed to preserve fat reserves for pregnancy. But when you’re trying to lean out post-kids or post-menopause, it works against you.
Conclusion
Subcutaneous fat — especially female abdominal subcutaneous fat — is genuinely one of the harder things to change about your body. The biology is stacked: fewer fat-releasing receptors, hormonal influences, and the simple reality that it’s the last reserve your body wants to give up.
But “hard” is not the same as “impossible.” The women who succeed are the ones who stop chasing 30-day transformations and commit to the long game: eating enough protein, moving their body consistently, sleeping properly, and managing stress. Not because it’s poetic — because those are genuinely the levers that move this particular kind of fat.
Frequently Asked Questions
1. How long does it take to lose subcutaneous belly fat?
Realistically, 3–6 months of consistent effort to see meaningful visible reduction, and up to 12 months for significant change in stubborn abdominal areas. This assumes a consistent caloric deficit, adequate protein, regular exercise, and good sleep. Expect the last few inches to take disproportionately longer — that’s biology, not failure.
2. At what age do you lose subcutaneous fat?
You don’t automatically “lose” subcutaneous fat with age — it actually tends to increase and redistribute. Muscle mass peaks in your 30s and declines steadily after that (sarcopenia), which lowers metabolic rate and shifts body composition toward more fat. After menopause, the abdominal region sees the largest increase. This makes proactive resistance training especially important from your 30s onward.
3. Does subcutaneous fat burn first?
No — typically the opposite. Visceral fat (the deep organ fat) is metabolically more active and tends to respond faster to diet and exercise. Subcutaneous abdominal fat, with its higher density of alpha-2 receptors, is generally last to go. You may see changes in your face, arms, and chest before your belly responds noticeably.
4. Why is my subcutaneous fat increasing?
The most common culprits: caloric surplus, declining muscle mass (especially if you’re not strength training), hormonal changes (perimenopause, postpartum), chronic stress and poor sleep, and high intake of processed foods. If fat is increasing despite a good lifestyle, a hormonal panel (checking thyroid, cortisol, estrogen) may be worth discussing with your doctor.
5. What is the fastest way to burn subcutaneous fat?
The combination of a moderate calorie deficit + high protein intake + HIIT and strength training + optimized sleep produces the fastest results that are also sustainable. There are no legitimate shortcuts. Medical options like CoolSculpting (cryolipolysis) can reduce localized subcutaneous fat but do not address the underlying metabolic conditions — and without lifestyle changes, fat returns. (Medical News Today)
6. How does subcutaneous fat feel?
It feels soft and squishy — the “pinchable” fat you can grab between your fingers. It’s pliable, moves when you poke it, and feels distinctly different from the hard, bloated feeling of visceral fat. If you can pinch it, it’s subcutaneous. If your belly feels hard and drum-tight despite not being visibly large, that’s more likely visceral.
The Reddit commenter was right. Subcutaneous fat is a bitch. But it does go. Eventually. Don’t give up.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before making significant changes to your diet or exercise routine.
← Back to all posts