How To Get Rid Of Hormonal Belly Fat In Women
Key Takeaways
- Hormonal belly fat — especially the stubborn lower pooch — is often driven by estrogen decline, high cortisol, or insulin resistance, not just calorie intake.
- Strength training 2–4x per week combined with 7–9 hours of sleep are among the most evidence-backed interventions for visceral fat reduction in women.
- Targeted supplements (ashwagandha, magnesium, omega-3s) and, for menopausal women, hormone replacement therapy (HRT), can meaningfully support fat loss when diet and exercise alone aren’t enough.

I want to start with something I read on Reddit that stopped me mid-scroll:
“I’ve lost 30 lbs, I’m at a healthy weight, I’ve done calorie deficits, intermittent fasting, weight training, more cardio… and that belly pooch is still there.”
That woman is 5’2”, 112 lbs, and 28 years old. By every conventional metric, she’s doing everything “right.” And yet — the belly stays.
If that sounds familiar, I need you to know: you are not failing. Your hormones might just be working against you in ways that no amount of extra cardio can override.
Let me break down what’s actually happening — and what I’ve learned actually moves the needle.
What Is a Hormonal Belly, Really?
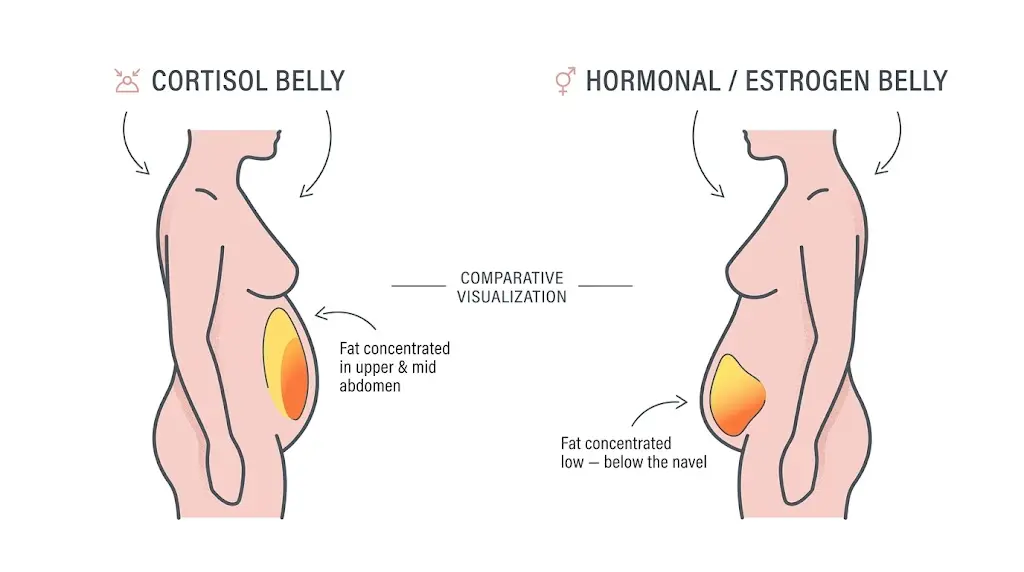
A hormonal belly isn’t just a regular type of belly fat. It’s visceral and subcutaneous fat that accumulates specifically in the lower abdomen as a direct result of hormonal imbalances — most commonly low estrogen, elevated cortisol, or insulin resistance.
Here’s how each one shows up:
Low estrogen (especially during perimenopause/menopause): As estrogen drops, the body shifts fat storage from the hips and thighs to the abdomen. A 2021 review in Climacteric confirmed that the visceral-to-subcutaneous fat ratio increases sharply after menopause — independent of total body weight.
High cortisol: Chronic stress keeps cortisol elevated, which directly stimulates fat storage in the abdominal region. Cortisol also raises blood sugar, promotes insulin resistance, and disrupts sleep — three things that compound belly fat. A study published in Psychoneuroendocrinology found that women with higher cortisol reactivity had significantly more central adiposity.
Insulin resistance: When your cells stop responding efficiently to insulin, excess glucose gets stored as fat — particularly visceral abdominal fat. The American Diabetes Association notes that this is one of the most predictive markers of metabolic disease in women.
The tricky part? These three drivers often overlap and feed each other. High cortisol causes insulin resistance. Low estrogen worsens cortisol regulation. Sleep deprivation accelerates all three.
What Does a Hormonal Belly Look Like?
A hormonal belly typically:
- Sits low on the abdomen — below the navel, not just around the waist
- Feels soft and squishy (unlike the harder “beer belly” that sits higher)
- Doesn’t respond proportionally to weight loss — you can lose 20 lbs and the lower pooch barely moves
- Is often paired with other hormonal symptoms: irregular periods, fatigue, mood changes, sleep disruption, or hot flashes
According to Medical News Today, hormonal belly fat in women is closely tied to estrogen dominance, low progesterone, and thyroid dysfunction — conditions that don’t show up on a scale but absolutely show up in the mirror.
How to Cure Female Hormonal Belly: The Evidence-Based Approach
1. Fix the Hormonal Root Cause First
Before you change a single thing about your diet or gym routine, get bloodwork done. Ask your doctor to check:
- Fasting insulin and blood glucose (insulin resistance panel)
- Estradiol and progesterone (estrogen balance)
- TSH, Free T3, Free T4 (thyroid function)
- DHEA-S and cortisol (adrenal function)
You cannot out-train an untreated thyroid disorder. You cannot out-diet estrogen dominance. Functional medicine approaches that start with root-cause testing consistently outperform generic weight-loss programs for women with hormonal belly fat.
2. The Diet Strategy That Actually Addresses Hormones
The goal here isn’t fewer calories. The goal is hormonal stability — keeping insulin low and steady, reducing cortisol triggers, and supporting estrogen metabolism.
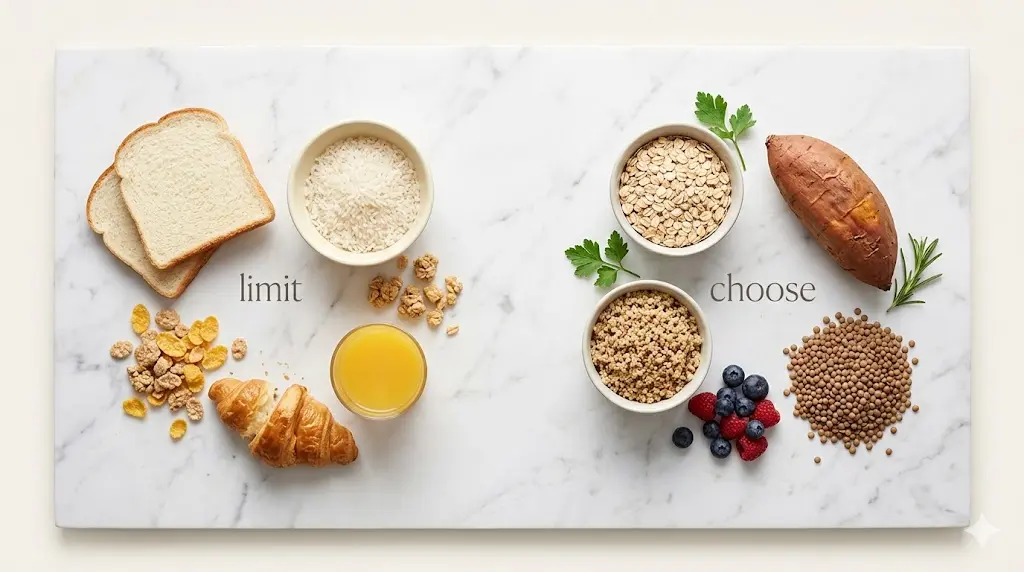
Cut refined carbs and added sugar aggressively. This is the most impactful dietary change for insulin-driven belly fat. A 2022 meta-analysis in Nutrients found that low-glycemic diets significantly reduced fasting insulin and visceral adiposity in women — independent of calorie restriction.
Eat 20–25g of protein at every meal. Protein blunts the insulin response of carbohydrates eaten in the same meal, keeps you satiated, and preserves muscle mass during fat loss. A 2020 study in Obesity showed high-protein diets (>25% of calories from protein) reduced visceral fat significantly more than moderate-protein diets in women.

Increase fiber — especially cruciferous vegetables. Broccoli, cauliflower, Brussels sprouts, and kale contain Indole-3-Carbinol (I3C), a compound that helps the liver metabolize estrogen more efficiently. This is particularly relevant for estrogen-dominant belly fat.
Limit alcohol. Alcohol impairs the liver’s ability to process estrogen, directly worsening estrogen dominance. It also spikes cortisol and disrupts deep sleep — hitting all three root causes at once.
Consider time-restricted eating (not aggressive fasting). A 2020 study in Cell Metabolism found that a 10-hour eating window — even without calorie restriction — reduced visceral fat, improved insulin sensitivity, and lowered blood pressure. Stop eating at 7pm, start again at 8am. That’s enough.
3. Exercise: What the Research Actually Says
Most women default to more cardio, more steps, more HIIT. What the body actually needs for hormonal belly fat is more muscle and less cortisol output from exercise.
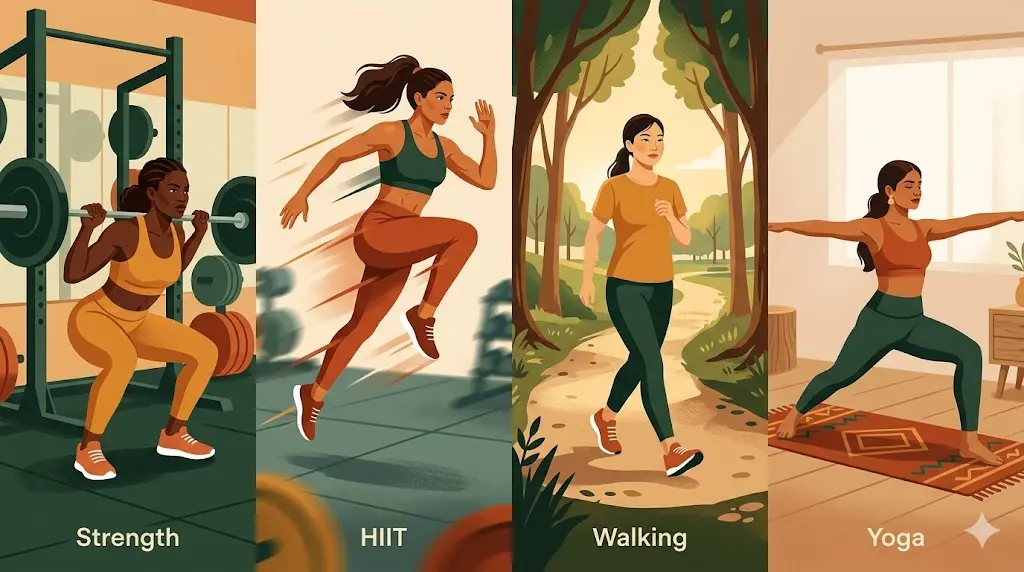
Strength training is the most important thing you can do. A 2021 review in Sports Medicine found that resistance training significantly reduces visceral abdominal fat in women, improves insulin sensitivity, and raises resting metabolic rate — even without dietary changes. Aim for 2–4 sessions per week using compound lifts (squats, deadlifts, rows, presses).
Add HIIT strategically — not daily. Two sessions of HIIT per week (20–30 minutes) is enough. More than that starts to chronically elevate cortisol. HIIT reduces visceral fat more efficiently than steady-state cardio — but efficiently means less is more.
Moderate cardio for cortisol recovery. Walking 30–45 minutes daily is one of the most underrated tools for hormonal balance. It’s anti-cortisol, improves insulin sensitivity, and doesn’t stress the nervous system.
Yoga and resistance training combined. A 2020 study in Menopause found that 12 weeks of combined yoga and resistance training significantly reduced cortisol levels and abdominal fat in perimenopausal women — hitting the stress axis and metabolic axis simultaneously.
4. Sleep: The Most Underrated Lever
Every hormonal system involved in belly fat — cortisol, insulin, estrogen, ghrelin, leptin — is regulated during sleep.
A 2010 study in Annals of Internal Medicine found that reducing sleep from 8.5 hours to 5.5 hours cut fat loss from a calorie-restricted diet by 55% — even though both groups were eating the same amount.
The target is 7–9 hours. Not as a suggestion — as a biological requirement for hormonal fat loss.
Practical non-negotiables:
- Consistent wake time (even on weekends)
- No screens 45 minutes before bed
- Keep your room cool (65–68°F / 18–20°C)
- Magnesium glycinate (200–400mg before bed)
5. Stress Management Is Not Optional
Cortisol-driven belly fat will not respond to diet and exercise if cortisol remains chronically elevated. You cannot outsmart the adrenal system with willpower.
Mindfulness-based stress reduction (MBSR): A 2016 study in Obesity found MBSR significantly reduced cortisol levels and abdominal fat in overweight women — no dietary change, no exercise change required.
Journaling and expressive writing: Research from UT Austin found that expressive writing about stressors reduces cortisol reactivity over time.
6. Supplements Worth Considering
Supplements are not a substitute for the above. But for some women — especially those under high stress or in perimenopause — the right supplements make a meaningful difference.
| Supplement | Dose | Evidence |
|---|---|---|
| Ashwagandha (KSM-66) | 300–600mg daily | 2019 RCT in Medicine: reduced cortisol, body weight, BMI, and food cravings |
| Magnesium glycinate | 200–400mg before bed | Improves cortisol regulation, insulin sensitivity, and sleep quality |
| Omega-3 fatty acids | 2–3g EPA+DHA daily | 2021 meta-analysis in Nutrients: reduced visceral and liver fat |
What to skip: Over-the-counter “fat burner” and “metabolism booster” products. Most lack credible clinical evidence, and several contain stimulants that chronically elevate cortisol — making hormonal belly fat worse.
7. Medical Options: HRT and Thyroid Treatment
Menopausal hormone therapy (MHT/HRT): For women in perimenopause or menopause, estrogen therapy has legitimate evidence for reducing abdominal fat accumulation and slowing the shift toward central fat distribution. This is a conversation worth having with your doctor.
Levothyroxine for thyroid dysfunction: If thyroid dysfunction is suspected (fatigue, hair loss, cold intolerance, unexplained weight gain), treatment can be life-changing. No lifestyle intervention adequately compensates for untreated hypothyroidism.
Conclusion
Hormonal belly fat is one of the most frustrating things a woman can deal with. Not because we’re lazy or doing things wrong — but because nobody tells us the full story: that our hormones are running an entirely separate conversation in the background, and no amount of extra crunches changes what’s being said.
Start with bloodwork. Build muscle. Sleep like it’s your job. Manage stress with the same seriousness you manage your diet. And be patient — because this kind of fat responds to consistency, not punishment.
Your body isn’t your enemy. It’s just been trying to protect you — with the wrong fuel.
Frequently Asked Questions
Does Hormonal Belly Fat Go Away?
Yes — but not by accident, and not quickly. Belly fat in women, especially hormonal belly fat, responds poorly to acute interventions (crash diets, intense short cardio programs) and responds well to sustained, multi-system lifestyle changes. Rapid weight loss spikes cortisol, which can actually make hormonal belly fat worse.
What Are the Signs of a Hormonal Belly?
Beyond the visual lower pooch, here are signs that your belly fat is hormone-driven:
- Fat accumulates disproportionately in the lower abdomen despite overall weight loss
- You have symptoms of hormonal imbalance (irregular periods, mood changes, fatigue, low libido, sleep disruption)
- You’ve lost significant weight but the belly pooch remains
- Fat storage shifted after a major hormonal event (starting/stopping hormonal birth control, postpartum, perimenopause)
- You carry stress chronically and struggle to switch off
What Is the 3-Day Hormone Reset?
The “3-day hormone reset” is not a medically recognized protocol. While some principles (cutting sugar, prioritizing vegetables, improving sleep) are sound, the idea that hormones can be “reset” in 3 days is physiologically inaccurate.
- Cortisol regulation responds to weeks of stress reduction
- Estrogen metabolism improves over months
- Insulin sensitivity shifts noticeably in 2–4 weeks with consistent dietary change
There are no shortcuts here — but the sustained approach works, and works well.
How to Get Female Hormones Back to Normal?
- Get tested. Know which hormones are actually out of range before spending energy guessing.
- Build muscle. Resistance training is the single most impactful exercise modality for hormonal belly fat.
- Sleep 7–9 hours. Non-negotiable. Sleep deprivation breaks every other intervention.
- Lower cortisol deliberately. Not as a lifestyle suggestion — as an active, daily practice.
- Be patient and consistent. Hormonal fat didn’t accumulate in a week. It won’t leave in one either.
This article is informational and does not constitute medical advice. Please consult a qualified healthcare provider before changing your diet, exercise routine, or supplement regimen.
← Back to all posts